Gastroschisis Causes, Symptoms, Treatment & Long-Term Outlook
Imagine receiving the news during a routine prenatal ultrasound that your baby has a serious but treatable birth defect. For thousands of families each year, that moment introduces gastroschisis — a condition in which the infant’s intestines (and sometimes other organs) develop outside the abdominal wall through a hole typically located to the right of the belly button. There is no protective membrane covering the exposed organs, unlike with other similar defects. This means that specialized care is needed right away after birth.
This complete guide talks about gastroschisis in simple, easy-to-understand terms. You will learn about the causes and risk factors, how it is diagnosed during pregnancy, modern treatment options, what recovery looks like, and things parents and caregivers can do to help make sure the best possible outcomes. This article gives you evidence-based information from trusted medical sources about emotional and practical realities of dealing with this diagnosis. It helps expecting parents seeking info, healthcare pros brushing up, or family supporting loved ones.
Table of contents
What Is Gastroschisis?
Gastroschisis is a congenital abdominal wall defect that occurs early in fetal development, usually between the fourth and tenth weeks of pregnancy. The abdominal wall fails to close completely, leaving a paraumbilical opening—most often to the right of the umbilical cord—through which the intestines protrude into the amniotic fluid. In some cases, the stomach or liver may also be exposed.
The condition differs from omphalocele, another abdominal wall defect, because the organs in gastroschisis lack a protective sac or membrane. This exposure to amniotic fluid can cause inflammation, swelling, and potential damage to the bowel, which influences both immediate management and long-term intestinal function.
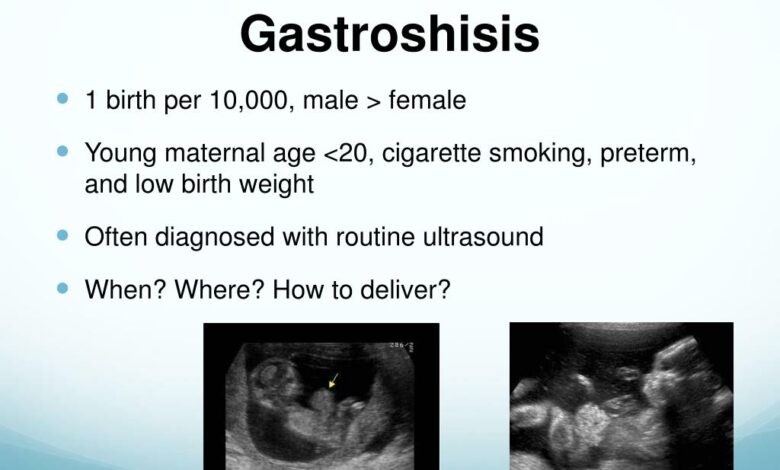
Gastroschisis affects approximately 1 in 2,000 to 1 in 5,000 live births, with rates appearing to rise in many regions worldwide. It occurs more frequently in younger mothers and is usually isolated, meaning it is not commonly linked to chromosomal abnormalities or multiple organ system issues, unlike some other birth defects.
Causes and Risk Factors of Gastroschisis
Most of the time, the exact cause of gastroschisis is not known. However, experts think it is caused by a mix of genetic factors and environmental factors. These factors halt normal abdominal wall closure or blood supply to that area during early embryonic development.
Known risk factors include:
- Young maternal age (under 20–25 years)
- Low socioeconomic resources or poor prenatal nutrition
- Maternal smoking, alcohol use, or certain medications (including some painkillers)
- Exposure to certain environmental toxins or infections
Importantly, gastroschisis does not typically run strongly in families, and the recurrence risk in future pregnancies is low—generally similar to the general population risk. This difference often makes parents who are worried about genetic inheritance feel better. Ongoing research is still looking into possible links to problems with blood vessels or problems with the growth of the right umbilical vein, but no clear cause has been found.
Prenatal Diagnosis and Monitoring
Doctors typically diagnose gastroschisis from ultrasounds taken in the second trimester, specifically from 18-20 weeks. What they typically see are loops of bowel that float in the amniotic fluid and outside of the abdominal cavity without any covering membrane.
Pregnant women will typically increase their visits to medical professionals to monitor their bowel issues, levels of amniotic fluid, and the progression of the fetus. Sometimes, examinations via ultrasound will reveal potential problems such as bowel loops that are excessive in width or thickness. These concerns can reflect inflammation or other issues like intestinal atresia (blockage).
It’s very important to plan the delivery. Many experts say that delivery should happen at a tertiary care center with a neonatal intensive care unit (NICU) and pediatric surgical expertise. Some centers recommend planned early delivery at 36 to 37 weeks if the lungs are mature, but this depends on the specifics of each case.
Immediate Care at Birth and Surgical Treatment
After birth, babies with gastroschisis need to be stabilized right away. The medical team quickly covers the exposed intestines with sterile dressings or a plastic “silo” bag to protect them from losing heat, fluids, and getting infected. The bag gently holds the bowel in place while it slowly returns to the abdomen.
Two main surgical approaches exist:
- Primary closure — If the abdominal cavity can accommodate the intestines without excessive pressure, surgeons return the organs and close the defect in a single operation soon after birth.
- Staged reduction with silo — More commonly used when the bowel is swollen or the cavity is small. The silo is suspended above the baby, and contents are gradually pushed back over several days as the abdomen stretches. Final closure follows once the organs are inside.
There has been an increase in the use of the plastic closure technique in the last couple of years for optimized cases in order to reduce potential scarring and anesthesia time. The focus of the post-operative care is to support the patient’s respiration, provide nutrition (with the initial phase consisting of intravenous feeds or total parenteral nutrition), prevent infection, and then slowly introduce feeds as the bowel starts to function again.
Long-Term Outlook and Potential Complications
With advances in neonatal care and surgical techniques, survival rates for isolated gastroschisis now exceed 90–95% in developed healthcare settings. However, challenges can arise:
- Short bowel syndrome or feeding difficulties if significant intestinal damage or resection occurs
- Intestinal atresia (blockage) in about 10–15% of cases
- Gastroesophageal reflux or motility issues
- Prolonged NICU stays, sometimes lasting weeks to months
Most children ultimately achieve normal growth and development, though some may need ongoing nutritional support or follow-up with pediatric gastroenterologists. Regular monitoring helps catch and address issues early.
Families can get a lot of help from support groups and organizations that help people with abdominal wall defects. These groups offer practical advice and a way to connect with others who have been through the same thing.
Actionable Steps for Expecting Parents and Caregivers
If you or someone you know has received a gastroschisis diagnosis, consider these practical steps:
- Seek care at a high-volume center experienced in managing abdominal wall defects.
- Ask detailed questions about the delivery plan, surgical approach, and expected NICU course.
- Prepare emotionally and logistically for a potentially extended hospital stay — arrange support for siblings, work, and daily needs.
- Learn basic signs of complications to watch for after discharge, such as persistent vomiting, poor weight gain, or abdominal swelling.
- Prioritize nutrition and avoid known risk factors in future pregnancies, while remembering that most cases are not preventable.
For healthcare professionals, staying updated on evolving techniques like minimally invasive or fetoscopic approaches is key. These (still largely investigational) ensure the best counseling for families.
Supporting Families Through the Journey
A diagnosis of gastroschisis brings sudden uncertainty and fear. But most families report that clear communication, compassionate care teams, and realistic expectations make an enormous difference. Early involvement of multidisciplinary teams—including neonatologists, pediatric surgeons, dietitians, and social workers—helps coordinate seamless care.
Parents often find strength in small daily victories: the first successful feed, removal of the silo, or discharge home. Celebrating these milestones while acknowledging the emotional toll is important for long-term family well-being.
Conclusion
Gastroschisis is a serious birth defect, but it can be managed well when it is diagnosed and treated in specialized settings. Today’s medicine is equipped to make the best of most situations, with issues that can be diagnosed before birth, performed in stages to include prolonged recovery. Families and caregivers, diagnosed with a condition, faced with options of risk, treatment, potential problems, can make decisions and offer support.
Remember that care is at a specialized center, that staging can be a good thing, and most children have the challenges of a full and active life ahead of them. It is understandable to be confused at the beginning, but that is where information and an effective care team can make a huge difference.
FAQs
What is the main difference between gastroschisis and omphalocele ?
Gastroschisis is a condition in which the intestines are exposed without a protective membrane. It usually happens to the right of the belly button as a single defect. Omphalocele is when organs are covered by a sac. It is more likely to happen with other problems or chromosomal issues.
How common is gastroschisis ?
It occurs in roughly 1 to 5 per 10,000 live births. Higher rates are seen in younger mothers and certain regions where incidence is increasing.
Can gastroschisis be prevented ?
There is no guaranteed way to prevent it. But avoiding smoking, and certain medications during pregnancy, along with good nutrition and prenatal care, may help lower overall risks.
How long do babies with gastroschisis usually stay in the hospital ?
Stays can be very different, but they usually last from a few weeks to a few months. This depends on how bad condition is, how well bowel is working, and how quickly person gets used to eating.